
The shoulder joint offers the greatest range of motion of any joint in the body. This incredible mobility, however, comes at a cost: vulnerability. The shoulder is a ball-and-socket joint, but the socket (glenoid) is quite shallow, much like a golf ball resting on a tee. When the shoulder’s stabilizing system is compromised, the shoulder can become loose, leading to a condition known as shoulder instability. This post will explore shoulder instability symptoms, along with causes and treatment pathways available to patients.
Key Takeaways
- Shoulder instability symptoms often include a feeling of looseness, slipping, or the shoulder “popping out.”
- Instability typically arises from a traumatic injury, but it can also develop gradually due to repetitive strain or underlying ligament laxity.
- Treatment frequently begins with non-surgical options, such as physical therapy, but surgical intervention may be recommended for recurrent or severe cases.
The Anatomy of Stability: Why the Shoulder is Vulnerable
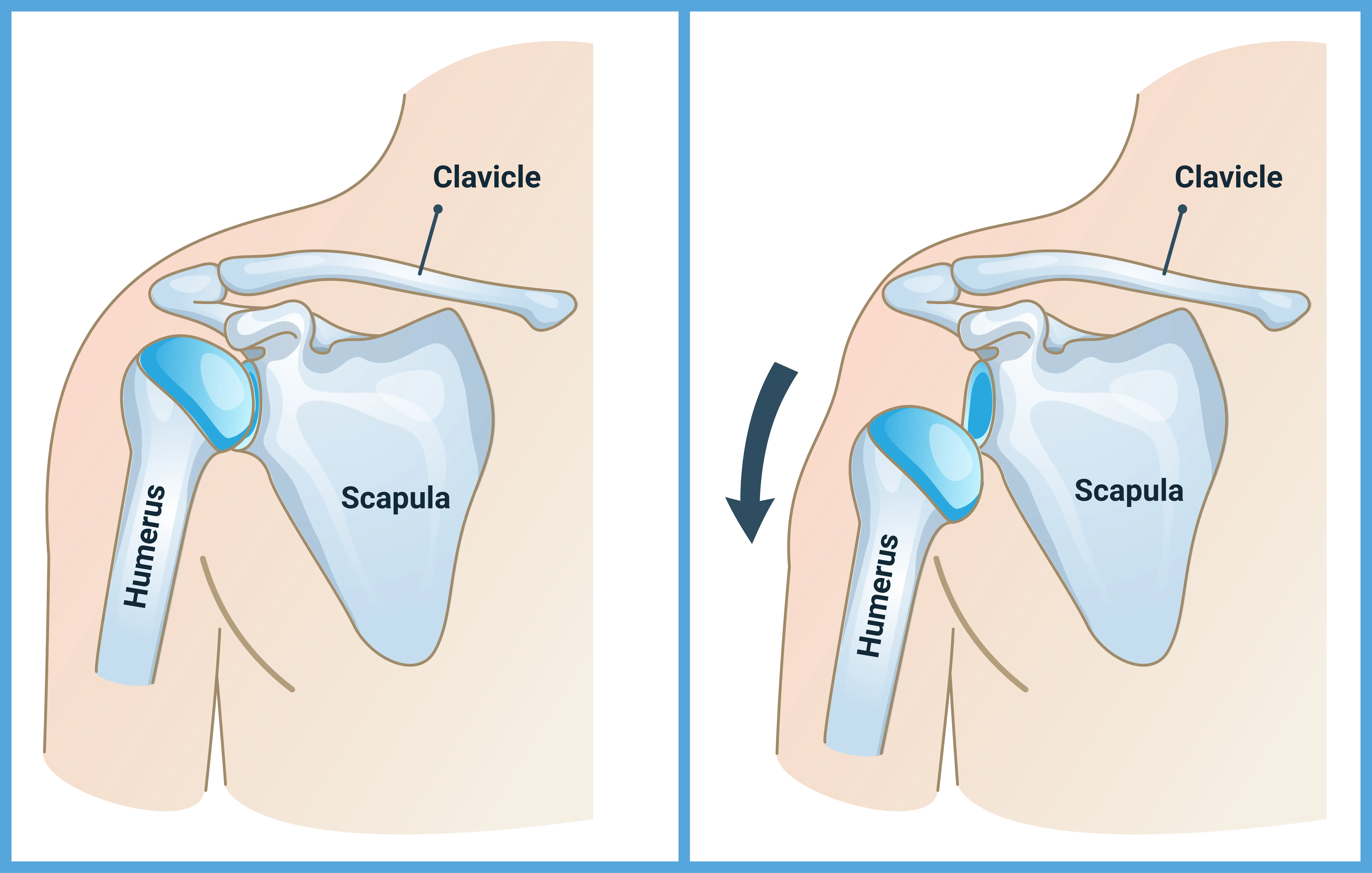
The shoulder is composed of three bones: the humerus (upper arm bone), the scapula (shoulder blade), and the clavicle (collarbone). The primary joint is the glenohumeral joint, where the head of the humerus meets the glenoid of the scapula. The glenoid is smaller than the humeral head. This mismatch is exactly what allows the shoulder to move so freely, but it also makes it vulnerable to instability.
Several structures compensate for this lack of bony stability. The labrum, a ring of cartilage around the glenoid, deepens the socket and provides a bumper. The joint capsule, a sac surrounding the joint, is reinforced by the glenohumeral ligaments. These ligaments act as the primary static stabilizers.
Dynamic stability comes from the rotator cuff muscles. They work constantly to squeeze the humeral head into the glenoid. When any of the static or dynamic stabilizers are damaged or stretched, the shoulder’s ability to remain centered can be compromised.
Recognizing Shoulder Instability Symptoms
The presentation of shoulder instability can vary widely among patients. Symptoms depend heavily on the severity of the injury and whether the instability is acute (sudden) or chronic (long-term).
Acute Instability: The Traumatic Event
Acute instability usually follows a significant traumatic event, such as a fall onto an outstretched arm or a direct blow to the shoulder. This may result in a full shoulder dislocation. A single shoulder dislocation may lead to future instability if the ligaments and surrounding structures are stretched or torn.
The most prominent symptom may be intense, immediate pain. The patient may feel a distinct pop or tear as the joint separates. Visibly, the shoulder may look deformed or “out of place.” The patient will likely be unable to move the arm at all. Numbness or tingling down the arm may also occur if nerves are temporarily stretched or compressed.
Chronic Instability: The Lingering Problem
Chronic instability is often more subtle. It may develop after an initial dislocation that was not fully rehabilitated, or it can arise from repetitive microtrauma, such as in overhead athletes. In these cases, the ligaments and capsule have been stretched out, or the labrum has been torn. The patient may not experience a full dislocation but rather a subluxation, which is a partial, temporary slipping of the joint.
Common Signs and Sensations
Patients frequently report a range of sensations that point toward instability. These symptoms may be exacerbated by placing the arm in certain positions, particularly overhead or when reaching back.
- Recurrent Subluxation: The shoulder partially slips out of the socket and then spontaneously reduces (goes back in). This can feel like a sudden, sharp pain followed by a quick return to normal, or simply a “clunk” or “pop.”
- Apprehension: A feeling of fear or anxiety that the shoulder will dislocate when the arm is placed in a vulnerable position, such as throwing a ball or reaching behind the head.
- Pain: While a full dislocation typically causes severe pain, chronic instability may cause a dull, aching pain that worsens with activity.
- Weakness: The patient may experience a perceived or actual loss of strength. This weakness often results from the body’s protective mechanism, where the muscles hesitate to contract fully for fear of causing a subluxation.
- Clicking or Popping: These sounds may indicate a torn labrum or other structural damage within the joint. The noise occurs as the humeral head moves over the damaged tissue.
It is important to note that these symptoms can overlap with other shoulder conditions. A professional evaluation may be necessary to pinpoint the exact cause of the discomfort.
The Diagnostic Process: Pinpointing the Problem
To diagnose shoulder instability, your doctor will likely combine a detailed patient history with a thorough physical examination and appropriate imaging studies. They may ask detailed questions about the onset of shoulder instability symptoms. They may want to know if a specific injury occurred, the direction of the dislocation, and how often the shoulder feels loose or “gives out.”
The physical examination generally involves a series of tests designed to gently reproduce the feeling of instability. Your doctor may also check for strength, range of motion, and any signs of nerve injury.
Imaging tests may provide evidence of any structural damage causing the instability:
- X-rays: Standard X-rays may be used to rule out associated fractures and to assess bone loss on the glenoid or the humeral head.
- Magnetic Resonance Imaging (MRI): An MRI is used for visualizing soft tissue structures. It may show tears in the labrum (Bankart lesion), damage to the joint capsule and ligaments, and tears in the rotator cuff.
Treatment Pathways for Shoulder Instability
The treatment for shoulder instability is highly individualized. It depends on the patient’s age, activity level, the type of instability (traumatic vs. atraumatic), and the extent of the structural damage. An experienced shoulder specialist will evaluate the condition, take individual health factors into consideration, and recommend an appropriate treatment path. The goal of treatment is to restore stability and help the patient return to their desired activities safely.
Non-Surgical Management
For many patients, particularly those with atraumatic or first-time traumatic instability without significant structural damage, non-surgical treatment can be the first line of defense. This is especially true in older patients (>30 years old) or those who are no longer participating in competitive sports.
Physical Therapy
Physical therapy is often a cornerstone of non-surgical management. A focus may be on strengthening the dynamic stabilizers, primarily the rotator cuff and the periscapular muscles (muscles around the shoulder blade). In the final phase of physical therapy, the patient may be guided through sport-specific or work-specific training to ensure the shoulder can handle the required loads and movements.
Activity Modification and Bracing
Patients may need to temporarily modify or avoid activities that put the shoulder in a vulnerable position. For athletes, this might mean taking a break from overhead sports. In some cases, a brace could be recommended to limit the range of motion and provide a sense of security.
Surgical Intervention
Surgery may be recommended when non-surgical treatment fails or when the initial injury involves significant structural damage that cannot heal on its own.
Arthroscopic Stabilization
Arthroscopy, or “keyhole surgery,” is a common surgical approach. It is a minimally invasive procedure performed through small incisions. The surgeon uses a tiny camera and specialized instruments to visualize and repair the damaged structures. A frequent arthroscopic procedure for shoulder instability is a Bankart Repair. The surgeon reattaches the torn labrum and the stretched ligaments back to the front of the glenoid bone. This can tighten the joint capsule and restore the integrity of the static stabilizers.
Open Stabilization Procedures
In cases of significant bone loss, an arthroscopic soft-tissue repair alone may not be sufficient. The shoulder may remain unstable because the socket is too shallow. In these situations, an open procedure may be required to restore the bony anatomy. A common open procedure for bone loss is the Latarjet procedure. This involves transferring a piece of bone (the coracoid process) along with its attached muscles (the conjoined tendon) to the front of the glenoid.
More recently, newer techniques have been developed to restore the bony support of the socket arthroscopically. An experienced shoulder surgeon can discuss whether this is an option based on your specific symptoms and anatomy.
Long-Term Prevention Strategies
Once stability is restored, patients may consider adopting long-term strategies to support their shoulder health.
- Consistent Strengthening: Continue a maintenance program focused on the rotator cuff and scapular stabilizers. These muscles are the body’s natural defense against instability.
- Proper Technique: For athletes, working with a coach to ensure proper throwing or serving mechanics can help reduce undue stress on the joint.
- Listen to Your Body: Any return of shoulder instability symptoms, such as a feeling of looseness or apprehension, should be taken seriously. Early intervention may help prevent a minor issue from escalating.
- Avoid Vulnerable Positions: Individuals with a history of anterior instability should be mindful of positions that combine abduction (arm away from the body) and external rotation (arm rotated outward).
Conclusion
Shoulder instability is a complex condition that can significantly impact a person’s quality of life. Whether the instability is the result of a single traumatic event or a gradual stretching of the joint, a tailored treatment plan may help restore function and confidence. From intensive physical therapy to advanced arthroscopic or open surgical techniques, modern orthopedic care offers a variety of solutions. If you suspect you are experiencing signs of shoulder instability, seeking a professional evaluation is a first step you can take.
Frequently Asked Questions
What is the difference between a subluxation and a dislocation?
A dislocation is a complete separation of the ball (humeral head) from the socket (glenoid). The joint typically remains out of place until it is manually reduced. A subluxation is a partial or incomplete dislocation. The ball slips partially out of the socket but then spontaneously returns to its normal position. Both are forms of shoulder instability.
Can shoulder instability heal without surgery?
Yes, in some cases. Non-surgical treatment, primarily focused on physical therapy to strengthen the surrounding muscles, may be successful, especially for atraumatic instability or a first-time traumatic dislocation without major structural damage. Surgery is typically reserved for recurrent instability or cases with significant structural damage.
What is a Bankart lesion?
A Bankart lesion is a specific type of injury that occurs during a traumatic shoulder dislocation. It is a tear of the labrum, the ring of cartilage that deepens the shoulder socket, at the front and bottom edge of the glenoid. This tear is a possible cause of recurrent anterior shoulder instability.
