
The shoulder joint offers an incredible range of motion, allowing us to perform countless daily activities. When pain and stiffness begin to limit this freedom, the experience can be frustrating and debilitating. Many patients find themselves asking, “What is a frozen shoulder and what causes it?” This condition, medically known as adhesive capsulitis, is a common yet often misunderstood source of shoulder pain and stiffness.
Key Takeaways
- A frozen shoulder, or adhesive capsulitis, involves inflammation and thickening of the shoulder joint capsule, leading to severe stiffness and pain.
- The condition typically progresses through three phases: the painful “freezing” stage, the stiff “frozen” stage, and the gradual “thawing” stage.
- Certain risk factors, including some medical conditions, may increase your risk of developing a frozen shoulder.
The Anatomy of the Problem: Defining Adhesive Capsulitis
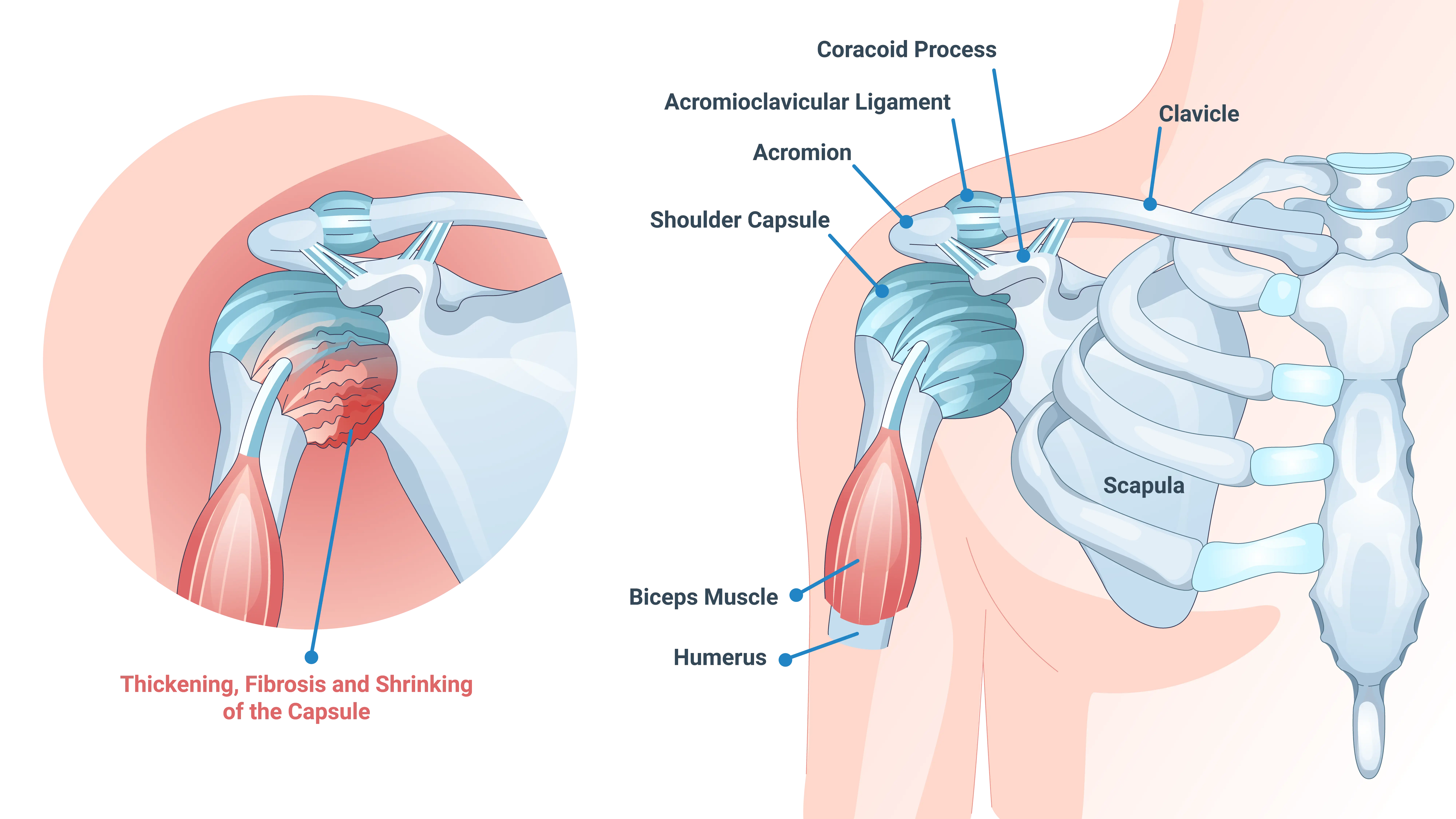
The shoulder is a ball-and-socket joint. The head of your upper arm bone (humerus) fits into a shallow socket (glenoid) in your shoulder blade. A strong, flexible tissue called the shoulder capsule surrounds this joint. This capsule contains synovial fluid, which lubricates the joint and helps it move smoothly.
In a patient with a frozen shoulder, the capsule becomes inflamed. Scar tissue, known as adhesions, then starts to form within the capsule. This process causes the capsule to thicken, tighten, and shrink. This restriction dramatically limits the space available for the humerus to move. The result is the characteristic pain and loss of motion that are associated with this condition.
The Three Stages of a Frozen Shoulder
Adhesive capsulitis typically develops slowly and progresses through three distinct stages. However, it is important to note that timelines may vary significantly between patients.
Stage 1: The Freezing Stage
This initial phase often lasts from around six weeks to nine months. You may first notice a gradual onset of pain, which worsens over time, especially at night or when you move your arm. As the pain increases, your shoulder slowly loses its range of motion. You might find it difficult to reach behind your back or lift your arm overhead.
Stage 2: The Frozen Stage
The “frozen” stage typically lasts between four and twelve months. During this phase, the pain may actually begin to improve. However, the stiffness generally remains severe, or it might even worsen. Moving your shoulder becomes extremely difficult. You may not be able to perform many routine activities. The range of motion is limited, but the intense, sharp pain of the freezing stage often subsides.
Stage 3: The Thawing Stage
This final stage marks the beginning of recovery. It usually lasts from five months to two years. In this phase, your shoulder’s range of motion may slowly start to improve. The pain continues to decrease. The capsule gradually loosens, allowing for more movement. While the recovery can be slow, many patients regain a significant amount of their original strength and mobility.
Unraveling the Mystery: What Causes a Frozen Shoulder?
The core question remains: what causes a frozen shoulder? Despite extensive research, the exact mechanism that triggers the initial inflammation is not fully understood in every case. Specialists frequently categorize the causes into two main types: primary and secondary.
Primary (Idiopathic) Frozen Shoulder
When no clear cause or preceding event can be identified, doctors may refer to the condition as primary or idiopathic adhesive capsulitis. It suggests that the condition starts spontaneously. The inflammation seems to begin without an obvious injury or surgical event. Patients may sometimes remember ‘tweaking’ their shoulder prior to symptoms starting, but often this is not a particularly memorable event.
Secondary Frozen Shoulder
A secondary frozen shoulder develops following a known cause or event. Several specific events or conditions can trigger a secondary frozen shoulder, including:
- Recent Surgery or Trauma: Any injury or surgery to the shoulder, arm, or chest can be a precursor. Patients often avoid moving the injured or operated arm due to pain. This lack of movement allows the capsule to stiffen quickly.
- Rotator Cuff Injuries: A tear in the rotator cuff can cause pain that naturally leads to reduced movement. This reduced movement can initiate the inflammatory and scarring process of adhesive capsulitis.
- Stroke: A stroke can cause partial paralysis (hemiparesis) of one side of the body. The affected arm may hang limp and be moved less frequently. This lack of active use can lead to a frozen shoulder.
- Other Conditions: Other issues like tendinitis or bursitis may cause enough pain to limit motion. Prolonged limitation of motion, for any reason, can increase the risk.
Who is at Risk? Understanding the Contributing Factors
While the exact answer to what causes frozen shoulder remains complex, there are several known risk factors. These factors make certain individuals more susceptible to developing the condition. Understanding these risks allows for earlier intervention and potentially better outcomes.
Systemic Medical Conditions
- Diabetes mellitus: Individuals with diabetes are more likely to develop frozen shoulder, and symptoms may be more severe.
- Thyroid disorders: Both hyperthyroidism and hypothyroidism are associated with a higher risk, possibly due to systemic inflammation or metabolic effects on connective tissue.
Demographic and Lifestyle Factors
- Age and gender: Most commonly affects adults 40-60 years old and is more prevalent in women. Hormonal changes, including those around menopause, may play a role.
- Immobilization: Prolonged lack of shoulder movement, such as wearing a sling after an injury or reducing activity due to pain, can increase risk.
How We Determine the Diagnosis
Diagnosing a frozen shoulder involves a thorough physical examination and a review of your medical history. During the physical exam, your doctor may check two types of movement: active (how far you can move your arm on your own) and passive (how far your doctor can move your arm for you). In a frozen shoulder, both active and passive range of motion are generally limited.
Imaging tests may be used to rule out other potential causes of your pain and stiffness:
- X-rays: Standard X-rays may be used to rule out arthritis or bone spurs.
- Magnetic Resonance Imaging (MRI): An MRI can provide detailed images of the soft tissues. In a frozen shoulder, the MRI may show thickening of the joint capsule.
- Ultrasound: Ultrasound is a quick and non-invasive way to visualize the tendons and joint capsule. It can help assess for inflammation and rule out other soft tissue issues.
The Path to Recovery: Treatment Options
Treatment focuses on managing pain and restoring motion more quickly. The goal is to minimize the impact on your daily life.
Non-Surgical Management
Many patients respond well to non-surgical treatments. These approaches are the first line of defense.
Physical Therapy: A skilled physical therapist can guide you through specific exercises. These exercises are designed to stretch the joint capsule and restore range of motion. Treatment often includes gentle stretching, range-of-motion exercises, and strengthening exercises. Consistency is key.
Medication: Nonsteroidal anti-inflammatory drugs (NSAIDs) can help manage the pain and reduce inflammation.
Steroid Injections: An injection of a corticosteroid into the shoulder joint may help reduce the pain and inflammation within the joint capsule. This reduction in pain can create a window of opportunity for more aggressive physical therapy.
Hydrodilatation: This procedure involves injecting a large volume of sterile fluid into the joint capsule. The fluid stretches the tight capsule. This technique can sometimes provide a more immediate improvement in motion.
Surgical Interventions
Surgery is typically reserved for patients who do not improve after several months of dedicated non-surgical treatment. The decision to proceed with surgery is always made on an individual basis. An experienced shoulder specialist can help guide if surgery is an appropriate treatment option for you.
Manipulation Under Anesthesia (MUA): This procedure is generally performed while you are asleep under general anesthesia. The surgeon gently but forcefully moves your shoulder. This movement breaks up the scar tissue and adhesions within the joint capsule. This is often done in combination with a capsular release (below).
Arthroscopic Capsular Release: This is a minimally invasive surgical procedure. The surgeon uses small instruments and a camera (arthroscope) inserted through tiny incisions. They carefully cut and release the tight portions of the joint capsule.
Surgical interventions are often successful in restoring full motion, but your body will then try to reform scar tissue. Because of this, after any surgical intervention it is important to get started in aggressive physical therapy immediately (often the same day or following day) to try to maintain the motion achieved during surgery. Make sure to discuss this plan with your doctor before the day of surgery so there is a plan in place.
Summary
Frozen shoulder is a condition of the shoulder joint capsule and can be triggered by a mix of systemic factors and periods of immobility. By understanding the three stages and committing to a comprehensive treatment plan, you can take better control of your recovery. While the process can be slow, many patients ultimately regain meaningful motion and experience significant pain reduction over time. Early recognition and proactive management often lead to smoother progress and help minimize long-term limitations.
Frequently Asked Questions
Is a frozen shoulder the same as arthritis?
No, a frozen shoulder is different from shoulder arthritis. Arthritis, such as osteoarthritis, involves the wearing down of the cartilage in the joint. This causes bone-on-bone friction. A frozen shoulder, on the other hand, is a problem with the joint capsule itself. The capsule thickens and contracts, restricting movement. While both can cause pain and stiffness, the underlying pathology is different.
Will I need surgery for my frozen shoulder?
Most patients do not require surgery. Non-surgical treatments are effective for the vast majority of cases. Surgery is typically considered when several months of non-operative treatment have failed to improve your range of motion.
Can I prevent a frozen shoulder?
Prevention may not be guaranteed, but you can take steps to help reduce your risk. One such preventative measure is to maintain full range of motion in your shoulder. For example, if you have an injury or surgery, you may opt to start gentle, doctor-approved exercises as soon as possible, as opposed to maintaining complete immobilization.
